
CCM, PCM, & RPM: A Virtual Safety Net for Rural Health Clinics Managing Chronic Care Patients
Optimize In-Home Patient Outcome | Reduce Hospital Readmissions and ER Visits | Increase Practice Net Revenue
In rural areas across the country, chronic illness carries a cost that rarely appears in clinical literature — the cost of access. In cities, care is measured in blocks or bus stops; in rural communities, it is measured in miles, hours, and the uncertainty of whether a clinic will still be open next year.
What are the Healthcare Challenges for Rural Patients?
For millions of Americans living in rural communities, managing a chronic illness is not just a health challenge — it’s a logistical one. The nearest specialist may be 60, 80, or even 100 miles away. Transportation is unreliable or non-existent. Time off work isn’t always an option. And the local clinic, if there is one, is often understaffed and overwhelmed.
The result? Rural patients with chronic conditions like heart failure, COPD, diabetes, and hypertension too often go unmonitored between visits, miss follow-up appointments, and end up in emergency rooms for situations that could have been avoided if caught sooner.
But something is changing. A powerful trio of Medicare-supported programs — Chronic Care Management (CCM), Principal Care Management (PCM), and Remote Patient Monitoring (RPM) — is transforming what chronic care looks like in rural America. Together, they form a complete support system that keeps patients connected to their care team, monitored in real time, and supported between visits — without requiring a drive to the clinic.
This article explores what each program does, who it’s designed for, and why the combination of all three may be the most important development in rural healthcare in a generation. But before diving into solutions, it’s important to understand just how wide the gap is.
The Rural Chronic Care Gap
Rural Americans are significantly more likely than their urban counterparts to suffer from chronic conditions, including heart disease, diabetes, and COPD. This population is also more likely to be older, lower-income, and uninsured or underinsured — factors that compound the difficulty of consistently managing serious health matters.
Rural hospitals have been closing at an alarming rate. According to The Chartis Center for Rural Health statistics reported in February 2026, a total of 206 rural hospitals have closed or converted since 2010, and 417 others are currently vulnerable to closure” (previously 182 and 432, respectively). Primary care physician shortages in rural areas are also well-documented. Specialist access is even more limited — in many rural counties, there is no cardiologist, no endocrinologist, and no pulmonologist within a reasonable driving distance.
The traditional model of chronic disease management — come in every three months, adjust medications, repeat — was never designed for patients who live an hour from the nearest clinic and can’t afford to miss a full day of work every quarter. That model leaves enormous stretches of time where a patient is essentially unmonitored and unsupported.
How CCM, PCM, and RPM Close the Care Gap
CCM, PCM, and RPM were each created to address a different dimension of this problem. Used together, they fill in every gap to ensure no patient is left behind.
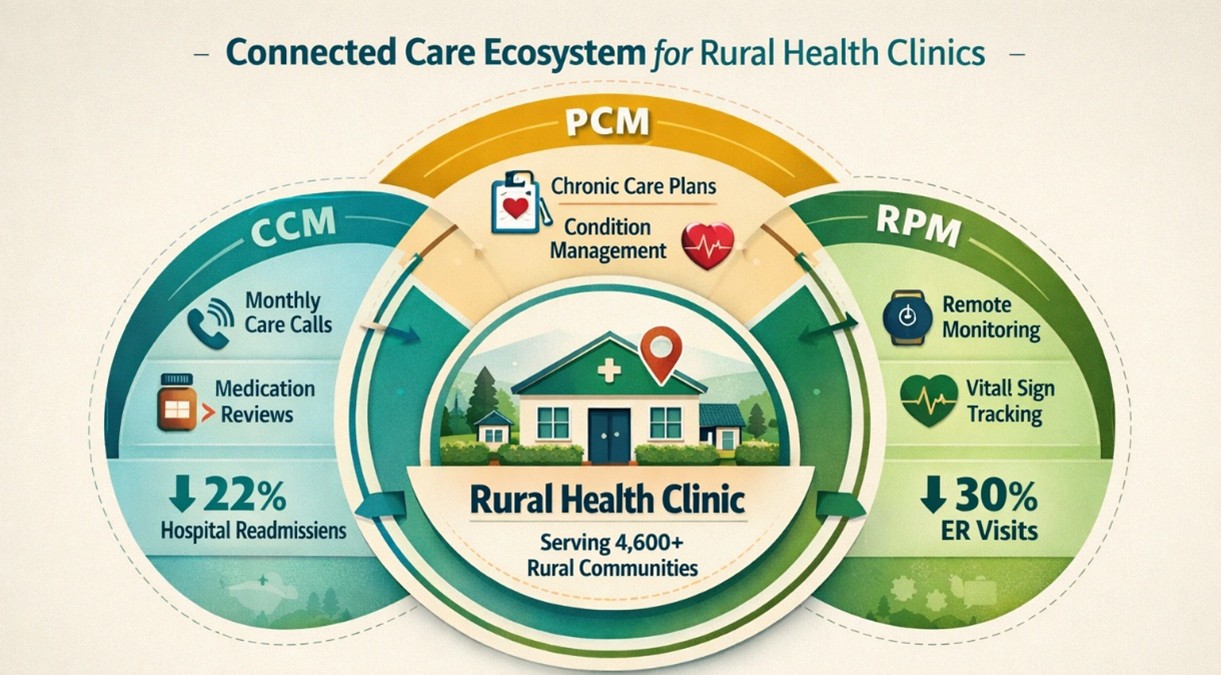
Source: CMS, Chartis Center for Rural Health, and DiaSante
Chronic Care Management (CCM): Coordination for Complex Patients
Who it’s for: Patients with two or more chronic conditions that are expected to last at least 12 months and place them at significant risk of decline or hospitalization.
CCM is perhaps the broadest of the three programs. It was introduced by Medicare in 2015 specifically to improve outcomes for patients managing multiple ongoing health conditions — the kind of patients who see multiple providers, take multiple medications, and require a level of coordination that a standard 15-minute office visit simply cannot provide.
At its core, CCM is a structured monthly care management service. Each month, a qualified care manager — often a nurse, medical assistant, or care coordinator working under a physician’s supervision — spends at least 20 minutes engaging with the patient. That touchpoint covers medication reviews, care plan updates, coordination between specialists, addressing social determinants of health, and proactive outreach to keep the patient on track.
For rural patients, CCM is particularly transformative because it replaces the follow-up visits that were not happening. A patient with diabetes and hypertension who used to go months without any clinical consultation now receives a monthly call. Medications are reviewed. Warning signs are discussed. Specialist referrals are coordinated. Gaps in care are identified before they become emergencies.
The results in rural populations have been significant. Studies consistently show that patients enrolled in CCM experience fewer hospitalizations, fewer ER visits, and better management of their primary conditions. For rural health systems operating on thin margins, fewer hospitalizations also mean a meaningful improvement in the financial sustainability of care delivery.
CCM is a program that rural practices can implement without dramatic infrastructure changes. It is billed under existing Medicare CPT codes, reimbursed monthly per enrolled patient, and can be delivered entirely by phone or telehealth — which means geography is not a barrier to participation.
Principal Care Management (PCM): Intensive Focus for Single-Condition Patients
Who it’s for: Patients with a single high-risk or complex chronic condition requiring intensive management.
PCM fills a critical gap that CCM alone cannot address. Consider a patient in rural West Virginia managing severe congestive heart failure. Their condition is serious, complex, and requires intensive monitoring and frequent clinical decision-making. But they only have one qualifying chronic condition. Under CCM’s eligibility criteria, they do not qualify. Without PCM, this patient is too sick for standard office-based care to adequately manage, but ineligible for the enhanced support CCM provides.
Introduced by Medicare in 2020, PCM is designed precisely for this population. It provides structured care management for patients with one serious chronic condition that is expected to last at least three months and requires a comprehensive care plan. Like CCM, it is delivered through monthly care management time, with a minimum of 30 minutes per month, and is reimbursed through dedicated CPT codes.
In rural communities, the number of PCM-eligible patients is substantial. Examples include the following:
- The COPD patient whose condition is deteriorating but who has not yet developed a second qualifying diagnosis.
- The diabetic patient who is newly diagnosed and requires intensive coaching and coordination to stabilize their blood sugar before complications develop.
- The cancer patient in active treatment who needs consistent care coordination but does not fit a two-condition CCM profile.
PCM ensures that these vulnerable patients receive the same level of proactive, structured support as those enrolled in CCM. It closes a significant eligibility gap and allows rural care teams to serve a broader swath of their chronically ill population under a sustainable, reimbursed framework.
Remote Patient Monitoring (RPM): Real-Time Data Between Visits
Who it’s for: Patients with chronic conditions that benefit from continuous or frequent physiological monitoring, including heart failure, hypertension, COPD, and diabetes.
If CCM and PCM are the coordination and management layer of rural chronic care, RPM is the eyes and ears.
RPM uses FDA-cleared devices — blood pressure cuffs, pulse oximeters, glucose monitors, weight scales, and others — to collect patient health data at home and transmit it automatically to the virtual care team. That data is reviewed regularly, often daily, by clinical staff to identify trends, flag concerning readings, and intervene before a patient deteriorates.
For rural patients, RPM is truly revolutionary. It means that a patient with congestive heart failure living 90 miles from the nearest cardiologist is not going 90 days between clinical touchpoints. Their weight is being tracked every morning. If it spikes by three pounds in 48 hours — a classic early warning sign of fluid retention and impending decompensation — a nurse calls that afternoon. A medication adjustment is made. A hospitalization is prevented.
RPM is reimbursed by Medicare under a set of CPT codes that cover device setup, patient education, data transmission, and the monthly clinical time required to review and act on the data. It has become one of the fastest-growing programs in value-based care due to its clinical and financial ROI:
- Continuous monitoring catches problems earlier
- Earlier intervention prevents hospitalizations
- Prevented hospitalizations save both the healthcare system and the patient enormous cost and suffering
In rural areas, the technology barrier that once seemed like an obstacle has also proven more manageable than expected. Many RPM devices connect via Bluetooth to a cellular hub that does not require a broadband connection. Patients in areas with poor internet access can still transmit data reliably. For older patients unfamiliar with technology, setup support and ongoing coaching help bridge the learning curve.
How Multi-Layered Chronic Care Programs Work for Rural Communities
Used in isolation, each of these programs delivers meaningful value. Used together, they create something that rural chronic care has never had before: a continuous, proactive, data-driven care ecosystem that brings care to the patient no matter where they live.
The RPM layer provides continuous physiological data — daily vitals that give the care team a real-time window into each patient’s health status. Trends are identified. Alerts are generated. Problems are caught early.
The CCM or PCM layer provides the clinical response infrastructure — the care managers, the care plans, the coordination between providers, and the monthly structured engagement that keeps the patient anchored to their care team. When RPM flags a concerning trend, the CCM or PCM team is the engine that responds, coordinates, and follows through.
These programs transform the care model from reactive to proactive — from waiting for the patient to show up in crisis to monitoring them continuously and intervening at the first sign of deterioration.
Consider a rural patient with heart failure and Type 2 diabetes. Under the integrated model:
- RPM monitors their daily weight, blood pressure, and blood glucose every morning
- CCM provides monthly care management calls, coordinates their cardiologist and endocrinologist, reviews their medication list, and updates their care plan
- If their RPM data shows weight gain and rising blood pressure in the same week, the CCM care manager calls, reviews symptoms, consults with the physician, adjusts the diuretic dose, and schedules a telehealth visit — all before the patient ever goes to the ER
This is not futuristic. This is happening today in rural communities across the country where forward-thinking health systems have implemented all three programs.
What This Means for Rural Health Equity
The availability of CCM, PCM, and RPM as a coordinated system of virtual healthcare delivery is more than a clinical advancement — it’s a health equity intervention.
For decades, the quality of chronic disease management available to a patient has been directly correlated with their proximity to an urban medical center. Patients in cities have easy access to care coordinators, disease management programs, specialist follow-up, and continuous monitoring tools. Patients in rural areas largely do not.
These three programs, fully reimbursed by Medicare and increasingly supported by Medicaid, change that equation. They do not require a patient to live near a hospital. They do not require a rural health clinic to have a large staff or sophisticated infrastructure. They simply require a virtual care team willing to engage patients proactively along with in-home technology tools that, in most cases, costs the patient nothing out of pocket.
A Coordinated Framework for Rural Patient Wellbeing
CCM, PCM, and RPM are not three separate programs — they complement each other to create the kind of comprehensive, continuous chronic care that rural patients have always deserved but rarely received.
CCM provides complex multi-condition patients with structured wraparound monthly support. PCM ensures that patients with a single serious condition receive the same level of intensive management. RPM fills the space between every visit with real-time data and early intervention.
No patient falls through the cracks. No warning sign goes unnoticed for three months. No rural zip code means settling for a lower standard of chronic care.
If you or a loved one is managing a chronic condition in a rural area — or if you are a provider looking to bring this model to your patients — the conversation about CCM, PCM, and RPM is one worth having today.
Did You Know? 2026 CMS Updates Expand Reimbursement for Rural Clinics
RHC and FQHC Billing Changes
The 2025/2026 CMS Physician Fee Schedule rules represent the most significant expansion in RPM/CCM billing flexibility for rural clinics in years. Effective January 2025, RHCs and FQHCs gained the ability to bill individual CPT codes for RPM, CCM, and PCM (rather than the bundled G0511), with full implementation and additional refinements under the 2026 PFS.
These changes make the CCM + PCM + RPM model more financially accessible than ever for rural health clinics operating on thin margins. DiaSante stays up to date with such policy changes to ensure you maximize your ROI.
Frequently Asked Questions
Q. Our clinic wants to launch an RPM program but lacks a dedicated care management team — what staffing models work for small rural practices?
A. RPM monitoring and CCM care management do not need to be performed by a physician or even on-site staff. CMS permits “incident-to” billing, which allows clinical staff such as RNs, LPNs, and medical assistants to conduct the monitoring and coordination under general supervision of a billing provider. Rural clinics commonly use three staffing models: hiring a part-time care coordinator shared across multiple providers, contracting with a third-party RPM/CCM vendor (like DiaSante) whose clinical staff performs monitoring on your behalf, or leveraging a regional health system’s care management infrastructure through a formal agreement. Whichever model you choose, documentation must clearly reflect the supervising provider’s involvement and the time spent must be logged accurately, as CMS audits these records closely.
Q. Are there patient consent requirements for RPM and CCM programs, and what must be documented before we bill?
A. Yes — both RPM and CCM require documented patient consent before services begin, and that consent must be captured in the medical record. For CCM, CMS requires that patients be informed of the scope of services, their right to stop participation at any time without affecting their other care, and any applicable cost-sharing (typically a 20% Medicare coinsurance applies unless the patient has a supplement). For RPM, consent must be obtained prior to device setup, and the initiation code (CPT 99453) can only be billed once per device, per patient. Verbal consent is permissible but must be documented with the date, staff member, and substance of the discussion. Given rural populations’ frequent reliance on family caregivers, clinics should also establish a protocol for authorized representatives when patients have cognitive or communication limitations.
Q. How do we handle patients who live in areas with poor cellular coverage — does that disqualify them from RPM?
A. Poor cellular coverage does not automatically disqualify a patient, but it does require a practical workaround strategy. Some RPM vendors offer devices that store readings locally and batch-transmit when the patient travels to an area with connectivity — a common pattern for patients who make weekly trips to town. Others support landline-based transmission or allow a family member’s smartphone to serve as the transmission hub via Bluetooth pairing. What CMS prohibits is manual patient entry as a substitute for automatic transmission, so any workaround must still result in electronic, device-generated data reaching your platform. Clinics serving frontier counties should request explicit confirmation from vendors about offline data retention and transmission protocols before signing a contract, and should document in the patient record how connectivity limitations are being managed.
Q. How much can our rural clinic realistically expect to receive per patient per month from Medicare, and is the return worth the administrative overhead?
A. Reimbursement varies by program and time tier. CCM pays roughly $62–$130+/patient/month depending on complexity and minutes logged. PPM pays approximately $57–$111+/month. RPM setup pays ~$19 once, with monthly monitoring codes ranging from ~$55–$75 for the first 20 minutes of clinical review. Rural Health Clinics and FQHCs bill these services under all-inclusive rates, which may differ from fee-for-service amounts — verifying your specific rate with your MAC before launch is essential.
Extend Your Reach with DiaSante — A Trusted Partner for Rural Health Clinics
Rural Health Clinics operate in unique settings, where they must serve patients with complex chronic conditions across large geographic areas, often with limited staff and resources. DiaSante is purpose-built for exactly this type of environment with custom-tailored solutions, from CCM, to PCM, to RPM, to eligibility verification and billing support.
Remote Patient Monitoring that works in rural areas. DiaSante’s devices use cellular technology with embedded SIM cards — no Wi-Fi or Bluetooth required — so patients in low-connectivity areas can still participate fully in their care. Our monitoring includes blood pressure, blood glucose, oxygen saturation, and weight.
Chronic Care Management, done for you. DiaSante’s care team handles outreach, enrollment, monthly check-ins, and real-time documentation — all directly inside your existing EHR. Implementation takes as little as 8 weeks, and the program is designed to ensure full CMS compliance from day one.
Generate revenue without adding headcount. DiaSante’s programs are structured to produce meaningful additional monthly revenue per enrolled patient, with no increase to your payroll. Our team provides billing documentation and CPT code recommendations each 30-day cycle.
A true extension of your team. Whether you need to ease staff workload, improve chronic disease outcomes, or both, DiaSante scales to fit your clinic’s size and goals.
Work with us to extend care beyond the clinic.
Interested in learning more about implementing CCM, PCM, or RPM services in a rural health clinic? Contact our care team to schedule a consultation.
_______________
Author Bio
M. Lee Holmes, FACHE, FACMPE, MHA/MBA
Chief Executive Officer, DiaSante
With over 25 years’ experience in healthcare, Lee has held leadership roles in integrated delivery systems and physician groups. His experience includes clinical, financial, and operations for physician groups, ambulatory surgery centers, urgent care, and hospitals.
About DiaSante
DiaSante is a remote patient monitoring healthcare solutions provider that is committed to revolutionizing the healthcare industry. The company’s aim is to improve health outcomes, grow clinical practices/systems, increase net revenue, and improve patient satisfaction.
Visit our website for general information about DiaSante.
Leave a reply